A previous version of this article appeared in Pulse, May 13th, 2016.
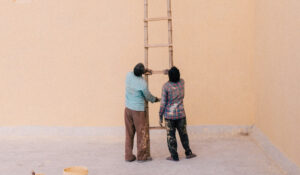
Normally we seek to avoid pain, whether associated with a known physical condition such as an injury or illness, or something more clearly perceived as psychic/emotional pain, such as despair, helplessness, anxiety. It is often easier to deal with acute pain, which by definition is time-limited. When chronic stress and tension, or a protracted injury or illness result in persistent and non-abating pain, the internal and external resources (e.g., friends and family) which we summon to help us meet the challenge of pain, may become relatively depleted. Chronicity makes us ragged around the edges, fatigued when constantly faced with more of the same, sometimes helpless and without hope that the pain can be managed effectively, or simply go away.
Various factors and dynamics exacerbate physical pain, expressed in symptoms and syndromes that may become chronic.
These include: (1) the mis-attribution of certain medical conditions to physical, mechanical or physiological structural changes, while overlooking the possibility that emotions may also lead to structural change (Sarno, 1991); (2) the resultant anxiety as to the medical diagnosis and prognosis and related treatment issues; (3) conflictual, repressed or isolated feelings that the person is not in touch with and lead to symptom formation; and (4) the dysregulation of the ANS, as typically seen in trauma, whether minor or major.
I will attempt to deal with each of these issues.
Despite an increasing awareness of the concept of holistic medicine, which sees the person as a whole and views the systemic connection of psyche and soma (body) as the unit of intervention, many physicians continue to view the body and its ailments as separate from the mind-brain. With increasing specialization, they are also tempted to focus on and treat the body part or system they have specialized in, referring the patient to other body part specialists as needed – forgetting that the whole is more than the sum of its parts, and not seeking to comprehend the overall picture. This fragmented view may exacerbate the patient’s anxiety, as he (or she) now have to contend with various medical issues, rather than an underlying cause that may account for the clinical picture.
Within the conventional medical model, emotions are not seen as inducing structural change. Back pain is a case in point. According to Sarno (1991), who worked for many years as director of outpatient services at the Rusk Institute of Rehabilitation Medicine at NYU Medical Center, there is a bias that “common pain syndromes must be the result of structural abnormalities of the spine or chemically or mechanically induced deficiencies of muscle.” (p. iix). Taking issue, he views the tension-based physical disorder he has named Tension Myositis Syndrome (TMS) as accountable for many of the symptoms his patients come in with, including fibromyalgia. Apparently a regional process, TMS is associated with tissue/nerve oxygen deprivation and may involve three types of soft tissue: muscle, peripheral nerve or tendon-ligaments. There is “a benign (though painful) aberration of soft tissue (and not the spine).” It may manifest itself gradually or even overnight, or be triggered (rather than caused) by a known physical event such as a fall. According to Sarno it is successfully treated via a combination of psychotherapy and psycho-education as to its emotional origins. Sarno argues convincingly that if the pain were structurally-based, it would not be expected to dissipate when treated by these means.
The role of emotion in generating or exacerbating physical pain.
According to Freud, we all deal with unavoidable, unconscious psychic conflict arising from opposing impulses and forces within us. Psychic conflict plays a part in character formation. It may be resolved in such a way as to allow for an acceptable degree of direct gratification, lead to sublimation, or result in symptom formation. The symptom is seen as a compromise between: “1) a partial, substitute gratification of drive derivatives and the unconscious fantasy wishes associated with them, and 2) the opposition of repressing and adaptive agencies, which results in a highly disguised, incomplete, and therefore consciously unrecognizable form of drive expression (Moore & Fine, 1983). According to these authors, “the suffering associated with most neurotic symptoms … satisfies the unconscious demand for self-punishment made necessary by the substitute gratification of conflictual drive derivatives achieved in the symptom.” (ibid). Simply stated, a little guilt and anxiety is better than a lot.
Moore & Fine attempt to address the complex issue of ‘choice’ of symptom:
“Particular symptoms, and the specific illnesses characterized by them, arise from the complex variations in the nature of the neurotic conflict, the differences in instinctual forces and the defenses employed, the nature and intensity of the external stresses and traumas, the strengths and weaknesses of the psychic apparatus and its component parts, and the character structure and life experiences of the individual who falls sick.” (p. 92, authors’ italics).
While illness may thus reflect a primary gain, that of the reduced anxiety associated with compromise formation, its ministration may unwitting lead to secondary gain. For example, a child is sick and nurtured back to health by a doting parent. Since none of us like to give up a good thing, perhaps later on, in adulthood, the ‘inner child’ may unwittingly express his (or her) need for ‘tender loving care’ by prolonging his illness beyond that strictly necessary.
In addition to the general underestimation of the possible role of emotion to both the evolution and maintenance of chronic pain, there is an additional oversight, which as a trauma therapist I must address.
What is often neglected, even by prominent physicians whose daily business consists of the clinical management of pain, has to do with the relative ‘contribution’ of trauma – experiences and feelings revolving around traumatic events, whether minor or major – to the symptoms and experience of pain.
And yet, like the title of van der Kolk’s (2014) important book, the body keeps the score. Even when not consciously remembered, our experiences are engraved, as it were, in the templates of our body-mind-brain – they shape these templates. This is part of what Solan (2015) has referred to as the memory traces of narcissistic processing. Starting with the very beginnings of life (presumably even in the womb) a cumulative learning process is initiated, in which the parent/s (caregiver) play a crucial role, for they provide functions that the infant cannot yet perform for himself. This learning process affects both our physiology and dynamic functioning of the structures of the brain, and the subjectivity of experience (the overall felt-sense of sensations, including feelings, memories, reflections and actual behavior). It prepares and immunizes us emotionally for what is to come (Solan, 2015) and allows our ego to devise coping strategies.
Born with the innate ability to experience nine innate affects (see Tomkins, 2008, in this regard), as we progress from being an infant to adulthood, and while attracted to the familiar and shunning and resisting that which is strange (Solan, 2015), we continuously accrue manifold experiences involving both danger and safety.
Initially experienced as strange and as representing a deviation from one’s body image, persistent painful sensations, by virtue of their repetitive nature, come to be processed as familiar, as part of our self. In autoimmune disease, the body/mind mistakenly attacks itself (Solan, 2015).
Biology becomes autobiography (Tomkins, 2008). If innate affects (biology) are like basic colors, autobiographical feelings are assembled or mixed in our own individual palettes (Kelly, 2009; Tomkins, 2008). Each of us has our own individual ‘scripts’ or ‘mental representations’ involving interactions with others (action schemes). At each moment in time, these scripts, scenes, and representations are colored by our unique, individual assembly of feelings and memory traces. They form our personal trauma and healing vortices (Ross, 2008). Our reservoir or library of experiences includes those characterized by physical and/or emotional pain (the trauma vortex) and the ways of assuaging them (the healing vortex), as well as what is generally referred to as ‘secondary gain.’
Like a pendulum that moves back and forth, our autonomous nervous system pendulates back and forth from one vortex to the other, from negative to positive experiences, from sensations of constriction and pain to those of expansion and well-being (Levine, Ross). It is important to continue adding to the positive experiences and to one’s resources, so they outnumber the negative. Sometimes, the metaphoric pendulum may become ‘stuck’ in the trauma vortex, and a preponderance of negative experiences may appear to wash out or cancel the positive ones, to cover them.
The healing vortex contains a reservoir of action plans and mental representations of successful coping upon which the person (ego) can rely when faced with new challenges. The more the pain patient is able to spend time in his (or her) healing vortex, and the greater and more versatile it is, this prolongs the pain-free moments, lessening the grip of pain.
Like prime numbers, sensations cannot be further divided. Our brain is equipped to process one sensation at a time. Both our innate affects and autobiographically-colored, personal feelings are comprised of embodied sensations – they have a bodily referent. For example, we know we are feeling anxious because our heart is pounding and we take in little air as we breathe; perhaps we have butterflies in our stomach or another visceral referent. When happy, we may feel light-hearted and bouncy, and our feet are ready to dance. In addition, sensations, the language of the felt sense (Gendlin, 1982) tend to be associated with sensory images (e.g., auditory, visual, tactile), feelings, thoughts, meanings, behaviors. Each sensation can be interviewed (Ross, 2008) and for each person, the resultant network or bundle of information is unique. This attempt to flesh out the cryptic messages of our sensations is important. Since in trauma there are often gaps in memory (e.g., retrieval difficulty) some of the current sensation’s channels (SIBAM elements) may no longer be directly linked to the original sensation/s at the time of the trauma (time zero). Becoming attuned to the communications or messages inherent in the sensations, listening to them and when possible, integrating their meaning, can often dissolve their grip on us, free us from their shackles.
I tend to believe that our ‘predisposition’ or proclivity to respond in a specific way at a particular moment in time is triggered or evoked by the seemingly random, fleeting encounter or ‘interface’ between (1) the templates or scripts that are stirred up by a certain stimulus (e.g., Solan’s memory traces of narcissistic processing), and (2) the particular constellation or balance that obtains at each moment between our trauma vortex and our healing vortex (Ross, 2008).
That this balance keeps changing from moment to moment means we can tip it in our favor: choosing to see either the half full glass or the half empty one, to use a well-worn metaphor. We can consciously and deliberately decide to tip the balance in favor of the healing vortex, by courting, and making room for positive, empowering, healing experiences and sensations. We can look for the silver lining in the cloud, the rainbow during (or immediately after) the outpour of rain. In short, we need to ‘collect’ experiences that make us feel good, that is, resources, and to notice how they make us feel. For example, we listen to our grandson read us a story he likes, or admire a flower we picked up during our morning walk, or help a friend or patient figure something out, while mindful of our body’s attendant sensations of expansion, the air that enters our lungs, how our shoulders expand. By making a point of anchoring each resource in our body, we are potentiating their effect on us. Try it.
Remember: each moment we spend in the healing vortex can help us counterbalance or counteract the magnetic pull of the trauma vortex, the destructive life forces, the sensations of constriction and imprisonment. By definition, there is a dynamism, an interplay between both vortices (“the polarity principle”), so that spending much time in the healing vortex can automatically trigger the traumatic vortex – and vice versa. The main thing is to be able to go back and forth (to ‘pendulate’) between vortices – rather than remaining struck in the whirlpools of the trauma vortex.
If we know that each sensation is short-lived, having a beginning, middle and end, and are able to remind ourselves of this when in pain – this should help dissipate some of the pain, in large measure exacerbated by anxiety. When we can predict it will relent (if only momentarily) we can try to savor this fleeting moment and perhaps amplify or prolong it by focusing our attention on it and tracking how it feels in our body. For example, is there now a sensation of expansion or relaxation, of more air entering our lungs? Which body parts are coming ‘online’ and announcing their presence, perhaps via a sensation of warmth or a pleasant sweat? Do we experience a nascent movement (micro-movements), say in our arms that want to stretch, or in our shoulders? Do we feel a pull to get up and stretch our legs? Track where this impulse starts, and see where it leads. Based on my work using these techniques, I can attest that they have a lot to offer patients in general, and the pain patient in particular.
Psycho-education and psychotherapy – especially a mind-body therapy such as somatic experiencing (SE) – can release much of the pain. However, once-a-week therapy may have its limits, although patients are taught and encouraged to utilize SE principles and techniques on their own. It is possible that a combined treatment approach involving additional modalities (for example, massage, yoga, cranio-sacral therapy, or neurofeedback) may be more effective in the release and management of residual pain. Research is needed in this area.
Chronic pain does not need to be a life sentence
References
Gendlin, E. T (1982). Focusing. New York: Bantam.
Kelly, V. C (2009). A Primer of Affect Psychology. Retrieved from http://www.tomkins.org/what…/vernon-kelly-a-primer-of-affect-psychology, 21December 2014. Also reprinted in The Art of Intimacy and the Hidden Challenge of Shame. Rockland, ME: Maine Authors Publishing.
Moore, B.E. & Fine, B.F. (1983). A Glossary of Psychoanalytic Terms and Concepts. New York: The American Psychoanalytic Association.
Ross, G. (2008). Beyond the Trauma Vortex Into the Healing Vortex. A Guide for Psychology and Education. Los Angeles, CA: International Trauma-Healing Institute.
Sarno, J.E. (1991). Healing Back Pain. The Mind-Body Connection. New York: Grand Central Life & Style, Hachette.
Scaer, R. (2014). The Body Bears the Burden. Trauma, Dissociation, and Disease. New York: Routledge.
Solan, R. (2015). The Enigma of Childhood. London: Karnac
Tomkins, S. (2008). Affect Imagery Consciousness. The Complete Edition. New York: Springer.
van der Kolk, B. (2014). The Body Keeps the Score. Brain, Mind, and Body in the Healing of Trauma. USA: Viking.
Ruth Shidlo, PhD, SEP. ITI, The International Healing-Trauma Institute. Dr. Shidlo is a trauma therapist and clinical psychologist based in Tel Aviv. A writer and editor, she is the author of The Rosebush Murders (2012) & Murder in the Choir (2016).