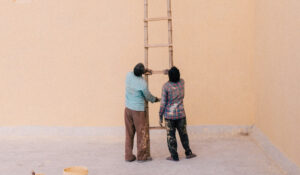

If you have felt threatened, whether when involved in military combat, apprehending potential terrorists, responding to an event as a first responder (e.g., paramedic, fireman, policeman) or upon witnessing such events as a civilian, your nervous system may have been overwhelmed by these experiences.
According to Levine (2008), in addition to war, events that may lead to PTSD include:
Levine also cites less obvious yet potential causes of trauma, which include seemingly ordinary events:
In certain cases, when this overwhelm is left untreated, people develop post traumatic stress disorder (PTSD). In part, this will depend on the amount of resources (internal and external) the individual has at the time, as well as their life circumstances and prior history (developmental history, trauma history).
Millions of veterans and civilians worldwide struggle with PTSD, and many have been helped to date.
Are thoughts and feelings regarding a life-threatening event that you were unable to deal with at the time upsetting you or creating problems in your life? Do you feel a loss of connection to others?
If your symptoms are extremely distessing to you, tend to disrupt your life, and last more than a few months, it is worth consulting a mental health specialist, such as a psychologist or psychiatrist. It is possible that you are living with PTSD.
According to the US Veterans Administration (VA), common PTSD symptoms include:
According to Levine (2008), the symptoms that will likely make their first appearance immediately following an overwhelming event include:
Levine goes on to list many other possible symptoms, some of which may manifest themselves early on, whereas others, years later. These symptoms (some of which were cited above re: the VA publication, yet too numerous to enumerate here) may come and go or remain stable (for more information, see website article, What is Trauma? Can it be prevented or healed? Part II). In time, symtoms may appear less and less connected with the original trauma.
A noteworthy symptom that deserves special attention, in part because it may create other problems when left unattended, is the compulsion to repeat or re-enact the actions that caused the problem in the first place. To cite Levine, “we are inextrictably drawn into situations that replicate the original trauma in obvious and less obvious ways.” (2008, p.19). An example may be a sex worker who was abused as a child.
Bear in mind that, more important than the actual symptoms that may manifest themselves, is how you choose to go about resolving them.
Ignore them and hope they’ll go away?
Feel that nothing and no one can help you cope?
Keep postponing or avoiding things you need to do?
Respond with reactive depression and/or anxiety?
Abuse alcohol and /or drugs to flee from it all?
Fight with your partner, family, co-workers, boss?
Tell someone how you feel?
Seek a support group?
Professional help?
Trauma is not a life sentence (Levine) and you can recover from it, or at the very least, manage your symptoms such that you regain control of your life.
PTSD is best treated by a trained trauma therapist, using trauma-focused treatment methods.
Dynamic psychotherapy or so-called “talk therapy” can be more effective when used in conjunction with a body-based therapy, such as Somatic Experiencing (SE).
Why? Because the body needs help in releasing residual energy that it recruited to deal with the threat, whether real or imagined, energy that, unused, remains trapped within it.
When, for a variety of reasons, we are unable to complete the instinctive action patterns of Fight and Flight responses, our default is paralysis and collapse, Freeze and Fold.
In the context of SE work, when we are able to discharge these hitherto truncated freeze responses, our brain is no longer in survival mode, and we regain our foothold in the present (see What is Trauma? Can it be prevented or healed? Part I).
It is important to sift through and separate the sensations, thoughts, images and feelings that may cause arousal and activation, and to learn how to track body sensations as they change. If you are able to swing back and forth (pendulate) between sensations of constriction and expansion, you are no longer stuck in habitual traumatic patterns. Moreover, you can become your own “personal scientist,” use your natural curiosity about your inner processes to help you get past feelings of helplessness or dread and other kinds of emotional pain.
In EMDR, attention is also given to the body and its sensations.
You will revisit certain traumatic memories and images and reprocess them and their attendant thoughts, feelings and sensations, while focusing on a movement, such as your therapist’s moving finger, or perhaps, tactile stimulation, such as tapping. Auditory stimulation may also be used.
Once the image no longer upsets you, you’ll work on adding a positive thought that will replace a previously held negative belief about yourself in that situation.
Often people invest much energy in avoiding dealing with aspects of their trauma. In PE, a form of cognitive behavioral therapy, you revisit your trauma-related memories time and again, and gradually learn to face up to and confront the situations that scare you. People have found that the more they aired their concerns and revisited their trauma, it lost its hold on them. Presumably, they learn that trauma-related memories and cues are not dangerous and need not be avoided.
In addition to imaginal exposure, treatment may also involve gradual in vivo (actual) exposure to such situations, for example driving, despite a frightening car accident.
When indicated, medication is best in conjunction with a course of psychotherapy, since it provides symptomatic relief but does not address the root causes of PTSD.
Levine, P. (2008). Healing Trauma. Boulder, Colorado: Sounds True.
VA Booklet. (May, 2019). Understanding PTSD and PTSD Treatment. (Last accessed, 27/4/2020, https://bit.ly/3eOv0Pf).
פיכולוגית קלינית ומטפלת בטראומה (SEP). בעלת תואר ראשון ושני בפסיכולוגיה מטעם אונ' בר-אילן ותואר שלישי בפסיכולוגיה קלינית מטעם ביה"ס לפסיכולוגיה מקצועית בסן דייגו.