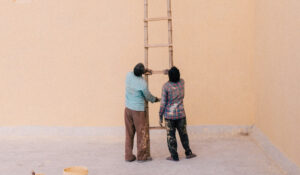

GIVEN THE MIND-BODY connection, our mental health affects our physical health and vice ver-sa. Depression is no exception. Many suffer from depression at least once during their lifetime. The length and severity of symptoms varies from person to person.
Generally speaking, it is best to intervene as soon as possible and attempt to nip the depression in the bud, before it becomes full blown.
Associated sleep difficulties and lethargy, commonly seen along the continuum of clinical depres-sion, may come to interfere with attention and concentration, as well as attendant processes of learning and memory.
The relationship between depression (e.g., major depression) and inflammation is currently receiving much attention, especially given potential implications for prevention and treatment.
Depression weakens the immune system and makes one more susceptible to viral infection and even diseases such as cancer. Another condition that may be affected by depressed mood is diabetes, which is reactive to stress. Research suggests that depressed people have three times the risk of de-veloping a cardiac event. While common for patients with coronary disease to exhibit transient sad-ness and depressed mood, when these persist and are accompanied by other symptoms, such as tear-fulness, social withdrawal or a lack of interest in previously enjoyed activities, it may be time for a professional intervention of some sort.
The experience of depression
Depression often involves a persistently sad and anxious mood, with attendant feelings of hopeless-ness, helplessness and/or worthlessness. There may be guilt feelings and one’s life may now appear unappealing, empty, devoid of interest. There may be a loss of interest and/or pleasure in previously enjoyed activities, including sex. It may be difficult to make a decision, especially when one tends to ruminate about things and doubt one’s self. Decreased energy and fatigue may also play center stage. Sleep disturbance (e.g., insomnia, early awakening, nightmares) and weight changes (e.g., due to loss of appetite or so-called “emotional eating”) may also emerge as part of the clinical picture.
The person focuses on the half-empty glass, rather than that half-full, as if putting on or wearing “negative glasses” — there is no light at the end of the tunnel, no hope for a better present or even a future, and the depressed person may feel helpless to change their life in a meaningful way. Feeling alone with it all, even when there are significant others in one’s life, is also part of the picture, and it is generally not helpful to remind the depressed person of their existence. Sometimes, depression may lead to fleeting thoughts of death by suicide or of dying, and these may culiminate in concrete plans or even a suicidal attempt. A cry for help should always be heeded and taken seriously. Better be safe than sorry.
In Israel, there is an Emotional First Aid Phone and Internet Hotline that can be contacted 24/7 as necessary (Eran = 1201). They are manned by volunteers and not fully fledged professionals. For professional help, please contact an outpatient mental health clinic or go the nearest ER.
How does depression come about?
There is no single known cause for depression. It reflects a combination of biological, psychological, genetic and environmental factors. The latter may be less familiar to the reader, and are thought to include air, noise, water and food pollution (e.g., food perseveratives, genetically-modified prod-ucts), electrical magnetic field pollution, and natural and manmade disasters.
Major life events such as loss of employment, coping with a difficult relationship, divorce and be-reavement, transitions such as Aliyah or relocation, major illness or other traumatic experiences, car-ing over time for someone who is dysfunctional or sick—all these are stressful for most of us, and may increase the likelihood of a depressive reaction.
Any stressful situation that overwhelms the ability to cope may result in depression.
The ways we respond to negative experiences, especially the tendency to ruminate or obsess over certain events and develop negative thoughts about one’s self tend to aggravate our mood disorder. So does our tendency to cut ourselves off from being socially engaged with others, an engagement that supports neurophysiological states promoting mental and physical health.
The regulation of physiological state, a core feature for every mental health condition, is affected when our engagement with others is lessened.
In fact, loss of social engagment and the co-regulation it provides for our nervous systems, results in a neurophysiological state that supports defensive behavior (such as fight or flight). If those around us cannot provide succour, our sympathetic nervous system kicks in, and we are in “survival mode.” When this becomes chronic, it tends to promote mental and physical disorders. Functional MRI studies show that the connectivity among parts of the brain involved in regulating mood, thinking, appetite, sleep and behavior is compromised. The bidirectional brain-gut relationship is also key.
It is important to realize that the person does not fully control his or her depressive reactions. The autonomous nervous system (ANS), which consists of three neural circuits (the sympathetic path-way and the two branches of the parasympathetic system i.e., the dorsal vagal and ventral vagal pathways), is constantly on the look-out for cues of safety and danger, which it communicates to the rest of the nervous system. This “neuroception” (a term coined by Porges, the proponent of pol-yvagal theory, to describe these processes) occurs outside our awareness. Whereas “fight or flight” are associated with sympathetic activity and mobilization, both “freeze” and “collapse” are associat-ed with dorsal vagal activity. Whereas there is some sympathetic mobilization in the freeze, collapse and total shutdown involve loss of muscle tone and immobiization.
The depressive reaction to stress— mediated via sympathetic activity and/or the dorsal vagal branch of the parasympathetic nervous system— can be understood as a response to a perceived lack of safety, that is, to danger and threat.
It is worth learning how to map one’s response patterns to cues of safety and danger,
identifying which state one is in, and then figuring out how to best transition or move through these states (whether alone or with others). It is not necessary to remain stuck in a dorsal vagal or immo-biized state.
Types of depression
Clinical depression is more that simply feeling blue. There may be a persistent low mood, accompa-nied by feelings of low self-esteem, decreased self-worth, low energy, and a decreased ability to experience pleasure (dysthmia).
Depression can manifest itself in reaction to childbirth (post-partum depression) or illness, or any of the stressors mentioned above. At times, depressive feelings may alternate with high spirits and even euphoria, as in bipolar conditions of various degrees.
Treatment
It is important to keep in mind that depression is not a sign of weakness or something that can be simply “willed away.”
Once a medical condition (such as a thyroid dysfunction, significant vitamin D deficiency, viral in-fection, or inflammation) is ruled out, you may wish to consider some form of psychotherapy, whether with or without a course of anti-depressant medication.
Some interventions, such as CBT, focus primarily on thinking patterns resulting in depressed mood and behavior. The premise is that if you can change your thinking, you will also change how you feel and behave.
Other treatment methods, such as SE or EMDR, utilize a more comprehensive, multimodal treat-ment approach, working directly with bodily sensations as well as emotional, thinking and behavior-al factors.
Recent advances in the treatment of depression include dietary regimes to alter the microbiome, electromagnetic devices capable of altering emotional brain circuits, and drugs that work on gluta-mate rather than on serotonin receptors.
It is always important to view the individual in the context of his or her social milieu, which in-cludes family and friends and other support systems, and to consider systemic interventions when necessary. Moreover, according to Porges, internalized family systems, also key in both the concep-tualization and treatment of depressive disorders, may be understood in the context of ANS func-tion.